
Most hospitals still manage discharge coordination through whiteboards and phone calls. A new generation of health systems is using predictive AI to recover thousands of lost bed-days and tens of millions in annual revenue.
The Bed That Should Be Empty Is Costing You a Fortune
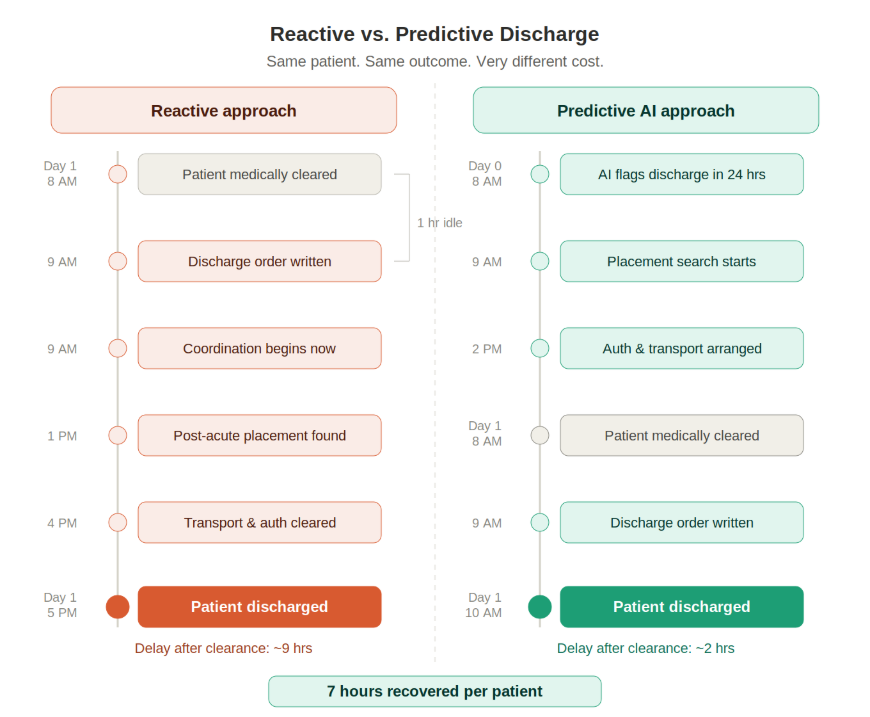
Right now, somewhere in your hospital, a patient is medically cleared to go home. The clinical team knows it. The attending knows it. And yet that patient will still be occupying a bed hours later because discharge coordination, post-acute placement, transportation, and paperwork are not moving in sync.
Patients who wait in the ED for more than a day before admission incur 10% to 20% higher costs than those admitted promptly. At Scripps Health in San Diego, more than 3,200 patients spent over 27,200 avoidable bed days at its five hospital campuses in a single year, up from around 10,000 days just three years prior.
This is not a staffing problem or a clinical problem. It is an operational intelligence problem. The question is whether your organization has the infrastructure to predict and prevent discharge delays before they happen.
Why Discharge Delays Are a Systemic Problem, Not a Scheduling Fix
Most hospital leaders have tried the same reactive fixes: more huddles, better whiteboards, daily bed meetings. These efforts help at the margins but do not prevent delays already in motion.
As the American Hospital Association notes, many discharge delays are not due to unresolved medical issues but to late-stage communication breakdowns, unclear expectations, and inadequate preparation for the transition out of the hospital.
For CIOs and CTOs evaluating operational AI investments, this distinction is critical. Discharge delay is primarily an information flow problem. Clinical readiness is determined hours before discharge occurs. Closing that gap requires real-time operational intelligence, not a better scheduling tool.
What Hospital Discharge Delays Are Actually Costing You
The financial exposure is significant. Between 11.2% and 30.7% of total hospital costs can be attributed to delayed discharges, representing $2,352 to $9,317 per delayed patient. Multiply that across a mid-sized health system and the annual figure runs into tens of millions, hidden inside inflated length-of-stay averages rather than appearing as a discrete line item.
Discharge Delay Cost Snapshot
- 11.2% to 30.7% of total hospital costs attributable to discharge delays
- $2,352 to $9,317 in costs per delayed patient
- $3.25B in avoidable costs per year at California hospitals alone
- 170M projected annual inpatient days by 2034, a 9% increase from current levels
The American Hospital Association's 2025 Cost of Caring Report identifies prior authorization requirements and post-acute placement shortages as the primary structural drivers behind delays that have doubled for Medicare Advantage patients since 2019.
The ROI Results Health Systems Are Producing Right Now
Predictive discharge planning is not theoretical. It is a production-grade capability running today with documented, auditable results.
According to a 2025 EpicShare case study on Parkview Health, shifting from reactive to proactive discharge planning reduced average length of stay by 0.54 days per patient, eliminated 2,450 excess hospital days, and saved $7.5 million in a single year.
That result came from one capability: knowing which patients were approaching discharge before the clinical team formally initiated the process. Care managers could arrange post-acute placement, transportation, and insurance verification in parallel rather than sequentially compressing the six-to-twelve-hour coordination cascade into time before the discharge order was written.
A peer-reviewed study from Cornell University found that an AI prediction tool deployed across seven hospitals reduced average length of stay by 0.67 days per patient and projected $55 to $72 million in annual revenue uplift. UnityPoint Health's EHR-integrated LOS model delivered $41 million in expense reduction and eliminated 38,000 excess hospital days over two years.
Three Operational Levers Real-Time Intelligence Unlocks
Real-time bed management
When bed status, discharge predictions, and ED volume are visible in a single operational view, bed management shifts from a telephone coordination exercise to a proactive capacity function. Charge nurses can see available capacity three hours out rather than discovering it reactively.
Post-acute placement acceleration
Predictive intelligence allows placement coordinators to begin the search a full day earlier, dramatically shrinking the window between clinical clearance and physical discharge, the single most common driver of avoidable bed days.
Surgical scheduling protection
Every delayed discharge is a blocked surgical case. When a patient occupies a bed past noon, the surgical patient scheduled for that bed tomorrow is at risk. Real-time operational intelligence makes that risk visible before it becomes a cancellation, protecting OR utilization and revenue simultaneously.
Why Most Hospital Systems Have Not Solved This Yet
The technology exists. The barrier is integration complexity. Hospital data environments are notoriously fragmented. EHR data lives in one system, transport tracking in another, post-acute placement and payer authorization in a third.
Building a real-time operational layer that unifies these sources and surfaces actionable outputs inside existing clinical workflows is fundamentally different from installing a point solution. Models that perform well in a clean pilot environment behave very differently against the real-time, incomplete data of a live hospital. Organizations that skip the data architecture work consistently end up with tools that staff do not trust and therefore do not use.
This Is the Operational Problem Connexr Was Built to Solve
Connexr is the AI solutions arm of RSA Tech Group, with 15 years of experience deploying AI and data infrastructure in regulated industries including healthcare, FinTech, and insurance. We are SOC 2, HIPAA, ISO 27001, and GDPR compliant across AWS, Azure, and GCP, with integration experience across Epic, Cerner, Salesforce, and major EHR platforms.
Every Connexr engagement starts with a data readiness assessment before a solution is proposed. We scope to your budget, architect around your specific workflows, and own the implementation from data pipeline through production deployment and ongoing managed services. We do not hand off and walk away.
Sources: Statistics in this article are sourced from publicly available research and industry reports including the American Hospital Association, EpicShare, Cornell University / arXiv, Health Catalyst, and NIH/PubMed Central. All sources verified April 2026.